Condition Basics
What is tongue-tie?
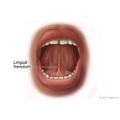
Tongue-tie (ankyloglossia) is a problem that is present at birth. It happens when the tissue that attaches the tongue to the bottom of the mouth (lingual frenulum) is too short. Tongue-tie can limit the movement of the tongue.
What causes it?
The cause of tongue-tie isn't always known. It can run in families or may occur in babies who have other problems that affect the mouth or face, such as cleft palate.
What are the symptoms?
Many babies with tongue-tie don't have symptoms. The tissue either stretches as the child grows, or the child adapts to the tongue restriction. But some children with tongue-tie have:
- Trouble latching on to the mother's breast and sucking. (Bottle-fed babies usually don't have feeding problems, because it is easy to get milk from the nipple of a bottle.)
- Gaps or spaces between the front lower teeth.
- Speech problems, because the tip of the tongue cannot rise high enough to make some sounds clearly, such as t, d, z, s, th, n, and l.
- Personal or social problems related to the restricted tongue movement, such as problems cleaning food off the teeth with the tongue. A child with tongue-tie may be made fun of by peers.
How is it diagnosed?
Your doctor will do a physical examination of your child's mouth and ask about his or her symptoms. In an older child or adult, the doctor may check the shape and movements of the tongue.
How is tongue-tie treated?
If your baby is younger than 1 year of age and has problems with feeding, the doctor may do a medical procedure (frenotomy) to clip the lingual frenulum. If your baby has tongue-tie and is feeding okay, you may choose to wait and see if his or her lingual frenulum stretches on its own.
While you wait and see, you can also:
- Talk to a lactation consultant if you are having breastfeeding problems.
- Consult a speech therapist if your toddler is having speech problems.
If tongue-tie causes speech problems or personal or social problems as your child grows, the doctor may do a frenotomy or a frenuloplasty. In this surgery, the doctor clips the lingual frenulum and closes the wound with stitches. The doctor may also teach your child how to do tongue exercises to improve tongue movement.
Most children don't need treatment because they adapt to the way their tongue is or the problem gets better as they grow.
Related Information
Credits
Current as of: November 14, 2022
Author: Healthwise Staff
Medical Review:
John Pope MD - Pediatrics
Kathleen Romito MD - Family Medicine
Current as of: November 14, 2022
Author: Healthwise Staff
Medical Review:John Pope MD - Pediatrics & Kathleen Romito MD - Family Medicine